In outpatient coding, coders are allowed to code from the pathology and radiology reports without the attending/treating physician confirming the diagnosis. The pathologist and radiologist are physicians and as long as they have interpreted the tissue or test then it may be coded.
Can you code a diagnosis from the lab report only?
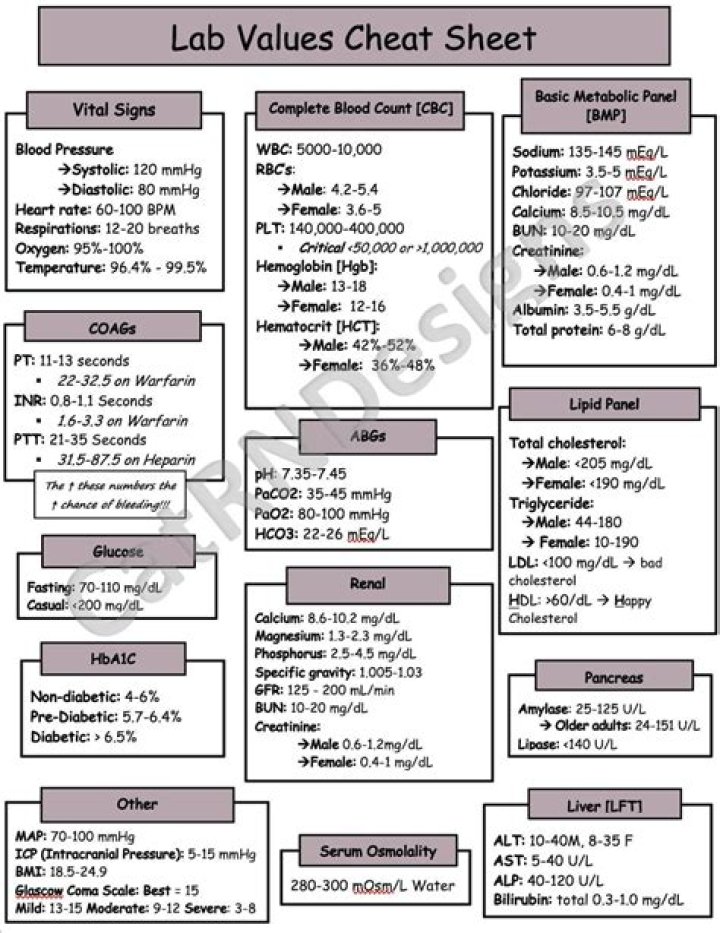
Since lab reports are not signed by a physician and are not interpreted by physicians, you cannot code from them. The Dr. reads the lab report and makes a definitive diagnosis or you can only code signs/symptoms and reasons for the tests if there isn’t a dx that can be used.
Can you code a clinical diagnosis?
Medical practices do not code suspected or possible diagnosis codes. Instead of using rule out, possible, probable, or likely diagnoses on claim forms for physician services, code the symptoms or complaint until a definitive diagnosis is made.
Can you code from pathology report inpatient?
Coding Clinic has clearly stated that in an inpatient setting, coders are not able to assign codes based on the pathology report without physician confirmation of the diagnosis. For example, breast cancer is documented, and the pathology shows mets to lymph nodes.Can I code a presumed diagnosis?
In the guidelines, CMS states the following: “Do not code diagnosis documented probable, suspected, questionable, rule out, compatible with, consistent with, or working diagnosis or similar terms indicating uncertainty.
Which Z code can only be reported as a first listed code?
A Z code is always the first listed code to report a newborn birth status. Z codes can be used in any healthcare setting.
What ICD 10 code for routine labs?
From ICD-10: For encounters for routine laboratory/radiology testing in the absence of any signs, symptoms, or associated diagnosis, assign Z01. 89, Encounter for other specified special examinations.
Can the inpatient coder assign a code based on the echocardiogram report?
In the inpatient setting, coders are not allowed to assign codes from diagnoses listed on diagnostic reports such as radiology, pathology, and echocardiogram (ECHO) even if a physician has signed the diagnostic report. … An ECHO is not a routine diagnostic study performed on every patient.Can outpatient coders code from lab results?
The pathologist and radiologist are physicians and as long as they have interpreted the tissue or test then it may be coded. … Outpatient coders may not code from laboratory reports unless the physician has made a notation regarding the findings with a diagnosis from the laboratory results.
How do you code radiology reports?- Heading (study name)
- Number of views or sequences (name of views – what was done)
- Clinical indication (reason for exam)
- Body of report (findings)
- Impression or conclusion (synopsis of findings)
- Physician signature.
- Diagnostic studies (plain films)
What documentation must be available to report the more specific code?
The goal is to report specific diagnosis codes when they are supported by the available medical record documentation and clinical knowledge of the patient’s health condition—and use unspecified codes only when they are the best choice to accurately reflect the healthcare encounter.
Do you code provisional diagnosis?
Under the newest edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), a provisional diagnosis is indicated by placing the specifier “provisional” in parentheses next to the name of the diagnosis. 1 For example, it might say something like 309.81 Posttraumatic Stress Disorder (provisional).
What is an example of a diagnosis code?
A diagnosis code is a combination of letters and/or numbers assigned to a particular diagnosis, symptom, or procedure. For example, let’s say Cheryl comes into the doctor’s office complaining of pain when urinating.
Can we code borderline diagnosis?
F60. 3 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
What type of coding uses a procedure code?
For some types of care, procedures are billed using CPT (Current Procedural Terminology) /HCPCS (Healthcare Common Procedure Coding System) codes, rather than ICD. CPT codes, also called Level I HCPCS codes, are used to bill physician services and they are copyrighted by the American Medical Association (AMA).
What is the ICD 10 code for rule out diagnosis?
Encounter for observation for other suspected diseases and conditions ruled out. Z03. 89 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
What is the ICD 9 code for abnormal labs?
2013 ICD-9-CM Diagnosis Code 790.99 : Other nonspecific findings on examination of blood.
What is the CPT code for lab work?
CPTDESCRIPTIONAverage Charge8557685576 PLATELET FUNCTION SCREEN$302.008500285002 BLEEDING TIME$446.008537985379 D DIMER (QUANT)$129.00DNA TEST COLLECTION/PREP FEE$159.00
What is the ICD 10 code for abnormal labs?
ICD-10 code R79. 9 for Abnormal finding of blood chemistry, unspecified is a medical classification as listed by WHO under the range – Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified .
What are Z codes in medical coding?
Z codes are a special group of codes provided in ICD-10-CM for the reporting of factors influencing health status and contact with health services. Z codes (Z00–Z99) are diagnosis codes used for situations where patients don’t have a known disorder. Z codes represent reasons for encounters.
Can Z71 89 be used as a primary diagnosis?
The code Z71. 89 describes a circumstance which influences the patient’s health status but not a current illness or injury. The code is unacceptable as a principal diagnosis.
Can you bill AZ code as primary?
Z codes may be used as either a first-listed (principal diagnosis code in the inpatient setting) or secondary code, depending on the circumstances of the encounter. Certain Z codes may only be used as first-listed or principal diagnosis. … Z Codes indicate a reason for an encounter and are not procedure codes.
Is the tip valid for facility related coding or for physician related coding?
Character 1Character 2Character 3SectionBody SystemRoot Operation
What is a diagnostic report medical?
A diagnostic report is the set of information that is typically provided by a diagnostic service when investigations are complete. The information includes a mix of atomic results, text reports, images, and codes.
In which setting would an ICD 10 PCS Procedure Code?
ICD-10-PCS is used only for inpatient, hospital settings in the United States, and is meant to replace volume 3 of ICD-9 for facility reporting of inpatient procedures. Due to the rapid and constant state of flux in medical procedures and technology, ICD-10-PCS was developed to accommodate the changing landscape.
Which term indicates an uncertain diagnosis?
H, “Uncertain Diagnosis” “If the diagnosis documented at the time of discharge is qualified as ‘probable’, ‘suspected’, ‘likely’, ‘questionable‘, ‘possible’, or ‘still to be ruled out’, or other similar terms indicating uncertainty, code the condition as if it existed or was established.
Which of the following providers is ultimately responsible for the final diagnosis quizlet?
involved in the care and treatment of the patient, so long as there is no conflicting information from the attending physician. If documentation from different physicians conflicts, the attending physician should be queried for clarification because he or she is ultimately responsible for the final diagnosis.
What is radiology coding?
by Coding Info on February 21, 2018 in CPC Exam tips – Radiology coding Guidelines. Radiology is a division of science that using imaging techniques like x-ray, Ultrasound, MRI/MRA, CT/CTA scan and PET scans to diagnose and treat a health condition.
What are the two components of radiology codes?
Most radiology services or procedures, although described by a single CPT code, comprise two distinct portions: a professional component and a technical component. The professional component is provided by the physician, and may include supervision, interpretation, and a written report.
How much do radiology coders make?
Annual SalaryMonthly PayTop Earners$84,500$7,04175th Percentile$73,000$6,083Average$59,860$4,98825th Percentile$41,500$3,458
How does medical documentation affect medical codes?
Thorough, detailed documentation leads to accurate coding, and accurate coding leads to appropriate and timely claims payments for hospitals and physicians. Most importantly, accurate documentation can lead to better, more effective patient care.